


Introduction
Stasis dermatitis (SD) is an inflammatory dermatosis of the lower extremities occurring in the setting of chronic venous insufficiency (CVI), a progressive venous disorder.1 SD is poorly characterized because it is typically considered a clinical manifestation of CVI, rather than a distinct disorder.1–3 CVI is considered the starting point for SD due to incompetent intrinsic valves in either the superficial (long and short) saphenous veins or deep veins, venous system obstruction (eg, deep vein thrombosis [DVT] or thrombophlebitis), arteriovenous fistula, failure of calf muscle pump (can occur with old age or prolonged standing) or valve destruction.1,4,5 The internationally recognized Clinical, Etiological, Anatomical, and Pathophysiological (CEAP) classification system defines SD as a distinct C4 venous disease in the context of FCVI progression, which ranges from C0 (no visible sign of venous disease) to C6 (active venous stasis ulcers).2,3,6,7
Abnormal venous flow of the lower extremities is observed in ~50% of individuals with SD, although the estimated prevalence of CVI varies depending on the study populations being evaluated,8 and reflects the differences in the distribution of risk factors, accuracy in the application of diagnostic criteria, and availability of diagnostic and treatment resources.9 A review of the literature indicated that the prevalence of CVI in the general population varied from <1% to 40% in women and from < 1% to 17% in men.8–13 SD typically occurs more frequently in older adults (>50 years) and women (particularly multiparous women) as well as patients with hereditary factors (including a family history) present.1,10,14 The estimated prevalence of SD in individuals aged >50 years of age in the United States is 6%–7% (approximately 15–20 million individuals), and as high as 20% by age 70.14–16
Understanding the epidemiology and risk factors of CVI is useful given the significant overlap with SD. Several studies identified risk factors associated with CVI, such as increasing age, female sex, and obesity.13,16–18 Additional risk factors for venous insufficiency (and, likely, the evolution into SD) include hypertension, heart failure, kidney disease, increased abdominal pressure (due to diseases including obesity, liver cirrhosis, and conditions such as pregnancy), sitting/standing for long periods, limited ankle motion (calf muscle pump dysfunction), and the use of certain medications such as calcium channel blockers, beta blockers, minoxidil, clonidine, hydralazine, methyldopa, estrogen, and nonsteroidal anti-inflammatory drugs.1,9,14,19–24 Traumatic injury to the leg as well as certain surgical procedures such as vein stripping and total knee arthroplasty have also been found to predispose patients to developing CVI and, subsequently, SD as part of the progression of the underlying venous insufficiency.14
SD is a chronic disease and, while treatments may alleviate symptoms and slow disease progression, there are no current treatments that target the underlying disease. SD is usually managed with non-pharmacologic and/or lifestyle changes; however, more severe cases may require topical or systemic therapies, or surgical interventions. Direct evidence regarding the treatment of SD is lacking and treatment options are often borrowed from therapy options used to treat CVI and other types of dermatitis.
This review discusses the diagnosis, treatment, and management of SD. A comprehensive search in MEDLINE and PUBMED databases was performed to identify relevant literature reporting on the treatment of stasis dermatitis.
Diagnostic considerations
1. Diagnosis of CVI
Chronic venous insufficiency (CVI) is typically diagnosed per clinical evaluation of physical characteristics of the affected skin together with a medical history that considers the risk factors noted earlier.25 Initial signs and symptoms of CVI may include brown macules and patches (due to burst capillaries and hemosiderin deposition), irritated pruritic dry skin, aching legs after standing, swelling on the inside of the lower leg (medial) and ankle varicosities.1,4 Corona phlebectatica, the fan-like dilated veins on the medial and/or lateral aspect of the foot, is recognized as a sign of worsening CVI and recently added to the CEAP criteria.6 As the disease progresses, flares of painful lipodermatosclerosis (LDS), atrophie blanche (white porcelain-like scars) and ulcerations with or without adjacent scars may be present (Figure 1).2,26 If the diagnosis of venous insufficiency is inconclusive, further examinations such as a venous duplex ultrasound to check blood flow or dermoscopy to check for glomerular vessels in clusters (ie, pathognomonic) may be helpful.1,27,28 A biopsy may be used to rule out malignancy (eg, Kaposi’s sarcoma and nonmelanoma skin cancers); however, biopsies are generally avoided because the affected skin is prone to chronic ulceration.4
_Acute,_(B)_chronic_stasis_dermatitis,_reproduced_with_permission_from_Dr._Itai_Ophir,_)
2. SD diagnosis/differential diagnosis
In contrast with CVI, the clinical diagnosis of which is usually straightforward, SD may be more prone to misdiagnosis because several cutaneous disorders can present with similar signs and symptoms.1 SD is primarily an eczematous disorder and presents with pruritus, erythema, crusting, and scaling, as well as vesiculation in the gaiter area. These clinical features are typically present on background of the CVI signs and symptoms described above (ie, edema, varicosities, etc). SD is often misdiagnosed as contact dermatitis or cellulitis. SD and allergic contact dermatitis are both eczematous disorders and therefore share similar exam findings. These two diseases may present simultaneously because of a high penetration of allergens through a damaged epidermal barrier in a patient with SD as well as contact with potential allergens applied to the skin to treat SD.1,26 Irritant contact dermatitis, a non-allergic inflammatory skin reaction, is another eczematous disorder that may present similarly, adding to the confusion and highlighting the need for the clinician to obtain a precise history and carefully examine the patient, noting, for example, patterns that suggest exogenous application of materials.26,29 In patients admitted to a hospital setting with presumed cellulitis, 30.7% were misdiagnosed; among them, 26% were diagnosed with SD after a dermatological consultation.30 The high rate of misdiagnosis is due to both SD and cellulitis presenting with erythema of the skin and swelling31; however, SD usually has a bilateral presentation and features of CVI and is not associated with systemic symptoms including fever and mild leukocytosis, both of which are common in cellulitis.1,31,32 The coexistence of SD and LDS, especially the acute painful variant, adds to SD’s misdiagnosis as cellulitis.33 SD is commonly mistaken for other cutaneous disorders, including nummular eczema, asteatotic eczema, pigmented purpuric dermatoses, psoriasis, and tinea corporis, as well as certain cutaneous neoplasms, including basal cell and squamous cell skin cancers.4,14
Misdiagnosis may lead to a lack of appropriate management and exposure to unnecessary drug therapy.31,32 As with SD, some of these conditions are managed with emollients to repair the skin barrier and topical corticosteroids to alleviate inflammation and pruritus4; however, compression therapy would most likely be absent from the regimen selected. Failure to address the underlying etiology of SD (ie, CVI) with the use of compression therapy would most likely result in the persistence of certain SD-related signs and symptoms; eventually, the patient would experience relapse and the disease would progress.1,34 It is important to refer patients for more advanced diagnostic procedures when the diagnosis is not clear.4 The involvement of a dermatologist who can perform patch testing and even a skin biopsy if needed could help improve diagnostic accuracy and decrease the use of unnecessary therapies such as antibiotics.30,32
Pathogenesis of SD
The pathogenesis of SD is poorly characterized, despite its impact on patient quality of life (QoL). Initially it was thought that the presence of a fibrin cuff surrounding dermal capillaries decreased the permeability of oxygen and nutrients, leading to the development of SD.35–37 As an extension of the fibrin cuff theory, the “trap theory” was developed. This theory suggests that various growth factors and inflammatory cells may become trapped in the fibrin cuff, leading to uncontrolled inflammation and the prevention of proper wound healing.35,38 Later, the fibrin cuff theory was disproven by studies which showed that fibrin cuffs can be found in other chronic ulcerative diseases in which venous oxygen tension was higher than that observed in patients with CVI.35,39,40 Because research on the etiology of SD is sparse and highly confounded by the investigation of other conditions that involve CVI, there is an imprecise understanding of the disease. Here, we present best evidence available regarding the treatment of SD while recognizing the need for better research on the exact mechanisms that underlie SD.
1. Venous hypertension
In the normal leg, increased venous pressure upon standing resolves with walking due to the contraction of the calf and foot muscles and efficient unilateral leaflike valves that support blood return to the heart. In people with venous hypertension, high venous pressures persist during ambulation.2,41 Venous hypertension due to venous reflux occurs secondary to incompetent venous valves (present in 70%–80% of cases), venous blood flow obstruction (eg, by thrombus) or muscle pump failure in the lower extremities,1,2,42 resulting in vessel wall distortion and venous valve incompetence.43 In the presence of incompetent valves, venous hypertension persists, leading to a chronic cycle of progressively worsening valvular incompetence and venous hypertension.4,42
2. Inflammation
The most probable cause of SD-related skin changes is the chronic inflammatory processes associated with venous hypertension, including the local accumulation of inflammatory cells, macrophages, and leukocytes,1,42–45 which result in further structural changes to venous walls and valves.42,43 One of the key processes leading to the progression of uncontrolled inflammation involves the extravasation of leukocytes across the vascular endothelium secondary to increased venous pressure.42,44–47 Intercellular adhesion molecule 1, vascular cell adhesion molecule 1, and their ligands are upregulated during the early stages of CVI (including SD), which drives the transmigration of leukocytes into nearby tissue, leading to skin damage and ulceration.48 These leukocytes infiltrate nearby tissues and secrete high levels of inflammatory mediators, perpetuating the inflammatory response.1,47 As observed in rat models of venous hypertension, leukocytes attach to the endothelium of the vein walls and valve leaflets, which leads to necrosis and/or apoptosis of the endothelium, fibroblasts, smooth muscle cells, and parenchymal cells of the venous wall.43 This could lead to further deterioration of venous wall structures and valve leaflets, causing a continued cycle of venous hypertension and subsequent inflammation.43 In addition, macrophages produce proteolytic enzymes, including matrix metalloproteinases (MMPs), which are thought to play a role in the breakdown of the extracellular matrix and impair healing.1,49,50
3. Histopathological changes
Several non-specific histological changes are associated with SD, including hyperkeratosis, spongiosis, and acanthosis. Spongiosis is mild in untreated SD but, if prominent, suggests concomitant contact dermatitis. Prolonged venous hypertension leads to extravasation and migration of macromolecules (fibrinogen and α2-macroglobulin, 2 plasma proteins which cause accumulation of collagen and subsequent thickening of the skin), leukocytes, and erythrocytes into the dermis.47,51 Deposition of hemosiderin, the breakdown product of hemoglobin from erythrocytes, can lead to hyperpigmentation and a persistent brown stain on the skin that may darken with time.4,42 Increased ferritin and ferric ion levels extravasated through hyperpermeable capillaries activate MMPs and perpetuate tissue damage.42 Studies have shown that increased venous hypertension is associated with overexpression of MMP-1, -2, and -13 without the inhibitory effects of tissue inhibitor metalloproteinases TIMP-1 and TIMP-2, which may result in hyperpigmentation, skin tissue damage, ulcer formation, and delayed healing.1,49 Hyperpigmentation and other SD-related skin changes may persist even when the underlying CVI is treated, making SD-related skin changes one of the more problematic SD-related symptoms to treat.1,42
4. Pruritus
SD-associated pruritus is likely nonhistaminergic because the use of antihistamines does not necessarily provide relief.47,52 Nonhistaminergic pruritus involves several itch mediators, including cytokines/chemokines, proteases and their receptor amines, neuropeptides and their receptors, ion channels, and immune cells.47 Interleukin-31 was recently identified as a potential target for skin conditions involving pruritus.53 Considering the potential pathogenesis of SD-related pruritus, targeting a decrease in mediators of pruritus may result in improved relief of pruritic symptoms compared to antihistamines.47 Pruritus is one of the most troublesome symptoms of SD and greatly impairs patient QoL. Furthermore, scratching due to pruritus aggravates wounds and increases the risk of skin infection and may result in skin thickening and lichenification.54
Treatment
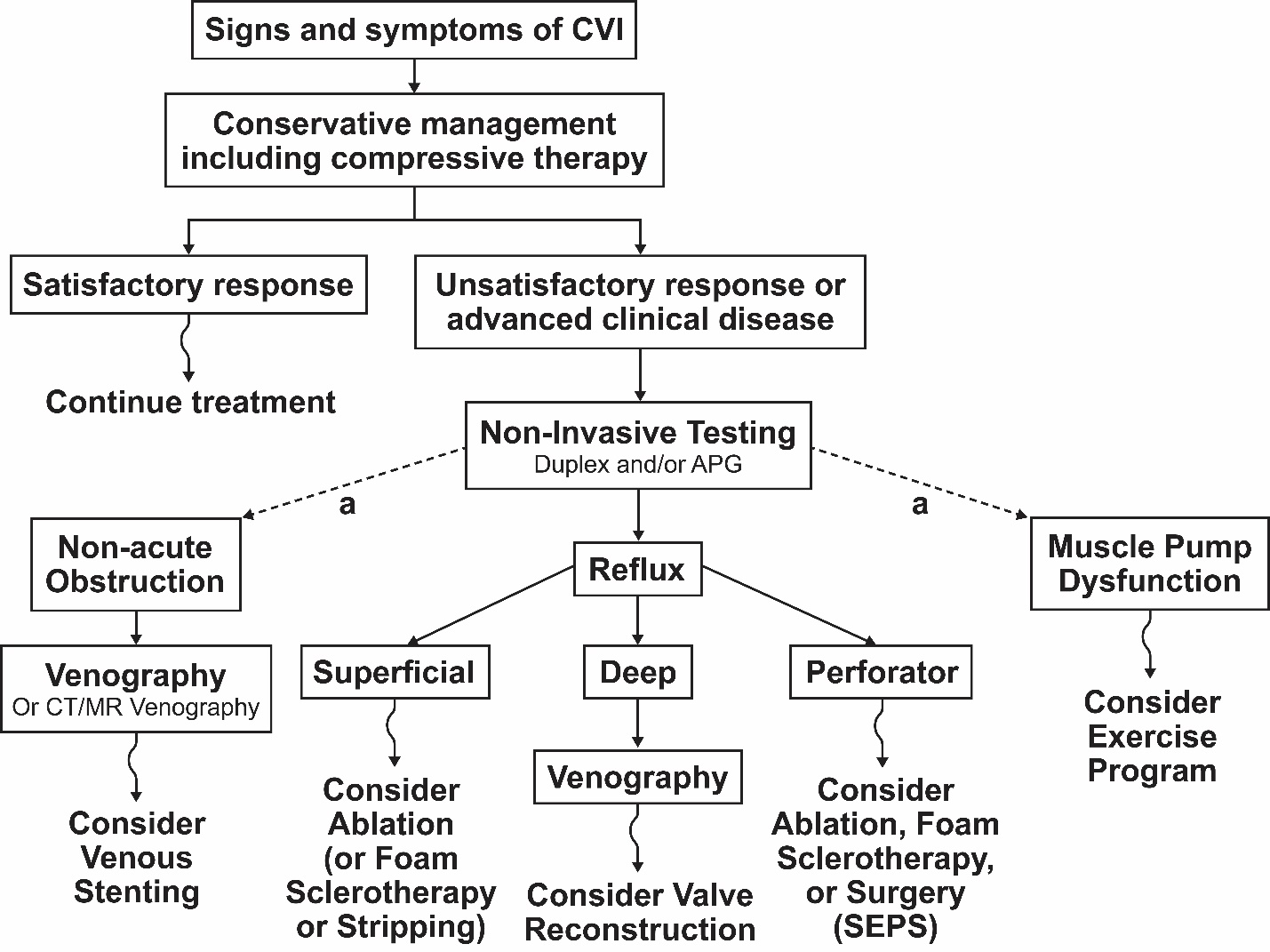
SD is undertreated and understudied, with few advocates within the health care profession. Multiple specialists may be involved, including dermatologists, geriatricians, and vascular surgeons, to treat the underlying venous insufficiency.55,56 The main goal of treatment in patients with SD is to address and minimize the clinical impact of the underlying venous insufficiency, alleviating downstream symptoms, including edema, pruritus, and inflammation, and improving pain, discomfort, and skin changes.1,7 However, despite the improvement in symptoms with treatment, venous insufficiency is a chronic, recurring condition and adult patients, who are typically older, often have other health conditions and risk factors that will worsen the disease (eg, heart failure, kidney disease, arthritis, and certain medications).1,7 A thorough understanding of pathogenesis of SD in the setting of CVI offers potential opportunities for treatment; however, given the imprecise nature of the research surrounding SD, targeted pharmaceutical interventions for SD are lacking. Initially, conservative approaches are frequently used and usually include compression therapy and, in some patients, adjunctive leg elevation, moisturization, exercise, dietary changes, and weight management, as well as addressing any known risk factors (Figure 2).26,57,58

First-line nonpharmacological treatments
1. Compression therapy
High-level compression therapy with stockings, compression wraps, bandages (Figure 3), pneumatic compression devices, or Unna boots, as well as non-elastic devices such as Hydro-boots form the cornerstone of treatment in SD.1,2,59 These devices create a pressure gradient by exerting a greater degree of compression around the ankle and a decreasing degree of compression upward along the lower extremities.59 Compression devices reduce ambulatory venous pressure and reverse venous hypertension, enhance venous return, and subsequently improve peripheral edema, pain, and skin changes.1,2,59 Moreover, through the restoration of normal blood flow, compression therapy assists in preventing disease progression and reduces the inflammatory processes, which are potentiated through venous hypertension.59–61

The overall pressure of compression devices is determined by factors such as the elasticity and stiffness of stocking material, the size and shape of the patient’s legs and their movements and activities.59 Pressures of 20–30 mmHg decrease ambulatory venous pressure and improve symptoms such as pain, swelling, edema, and stasis skin changes, and pressures of 30–40 mmHg are used for more severe cases in which ulcers may be present (Table 1).62
Although there is a lack of randomized controlled trials (RCTs) assessing the efficacy of compression therapy for the treatment of SD versus no compression, there is high-quality evidence that compression therapy increases the rate of ulcer healing and improves pain compared to SD that is not treated with compression.62 A systematic review concluded that graduated-compression stockings may prevent the recurrence of venous ulcers and that high-compression stockings may be more efficacious than those of moderate compression. Patients with edema, weeping, and other skin changes were also found to have benefited from the use of compression therapy.59 Evidence substantiating the role of compression therapy in CVI in addition to strong clinical experience suggests a role in SD treatment.
Although the use of compression therapy is considered the cornerstone of treatment for venous disease, only ~50%–60% of patients are adherent.1,63,64 Compression therapy is difficult to self-manage, with bandages being more difficult to use than stockings.1,63 When using bandages, the patient may need to see an appropriately qualified health care professional multiple times per week for proper application, which may be difficult due to a lack of time or transportation problems.63 Although the use of bandages is associated with higher efficacy in terms of improvement in SD-related symptoms, stockings are associated with improved adherence.1 Wraps are reusable and easily replaced or adjusted by the patient; however, obesity and a lack of manual dexterity may limit self-management.65,66 Patient adherence with compression therapy is influenced by numerous factors, including discomfort due to a poor fit, a sensation of heat in the legs, and exacerbation of itching as well as a negative self-image associated with the appearance of compression devices at work, school, and everyday life.67–69 In addition, the financial burden associated with the cost of compression devices and patients’ inability to put on the stockings and take them off because of frailty, lack of mobility, or obesity may also negatively influence adherence.1,34,69 A lack of understanding of SD chronicity and the consequences of nonadherence to prescribed SD management regimens and barriers to motivation are considered key contributing factors to poor treatment adherence. Compression therapy is vital in the management of SD; therefore, finding ways to improve adherence is important.2,34,70 Adherence can be improved through patient education, proper fittings, and patient follow-up; however, time and resource constraints on health care professionals often make this difficult.1,34,70
In some cases, the use of compression therapy may not be possible. Contraindications include allergy to stocking material, recent skin grafts, extreme leg deformity preventing correct fit, suspected or proven peripheral arterial disease, or severe peripheral neuropathy.59 Compression on a leg with compromised arterial circulation can increase the risk of ischemic damage.59 For these patient groups, alternative treatment options need to be considered.
2. Leg elevation
Leg elevation is mainly used for mild cases of SD.1 When the legs are elevated, there is less gravitational hindrance preventing blood flow. Consequently, leg elevation helps improve venous pressure, increase blood flow (improving microcirculation) and oxygen delivery, and reduce edema.71
Leg elevation in patients with CVI is associated with significantly higher laser Doppler fluximetry, higher blood cell velocity, and a significant reduction in lower limb edema. In addition, patients who practiced leg elevation were less likely to have ulcer recurrence than those who did not.72
3. Wet-to-damp gauze dressings
Weeping lesions can be treated with wet-to-damp gauze dressings soaked in water or with a drying agent.73 Moist occlusive dressings control exudate and promote epithelial cell migration and are also believed to provide symptomatic relief for pain and pruritus. A moist environment accelerates wound healing because it facilitates debridement of the wound and removes the surface bacteria.74 Wet wraps rehydrate dry skin and enhance the absorption of topical treatments such as corticosteroids.75 These types of dressings are best used after bathing, moisturizing, and applying medication.
4. Lifestyle changes
Modifiable risk factors can often be managed and minimized through lifestyle changes; however, maintaining these changes is difficult. There is often a high level of reduced treatment adherence due to cost, inconvenience, a slow rate of improvement in symptoms, and lack of understanding of these types of treatments. All these factors may demotivate patients.1,34,69
Sedentary lifestyle
Patients with a sedentary lifestyle have been found to have decreased blood flow compared with patients who are active and exercise.58 Exercises are recommended for patients with CVI to increase the movement of the ankle joint and strengthen the calf muscle pump, thereby improving blood flow and preventing disease progression; however, efficacy is dependent on adherence.4,58,76 As CVI affects a significant proportion of the older adult population (≥50 years), advanced age and increased pain secondary to the progression of venous insufficiency often limits mobility and, thus, the ability to exercise.1,77
Conversely, prolonged periods of standing can result in venous pooling, worsen venous insufficiency and compromise overall vein integrity.71 Thus it is important to balance an active lifestyle with rest and leg elevation.
A sedentary lifestyle contributes to the development of other risk factors for CVI, such as obesity. Lower limb venous flow has been found to be significantly reduced in the obese patients, and obesity can also predispose patients to the development of metabolic syndrome and venous stasis, which may trigger CVI.18 Dietary changes (including a low-salt diet to reduce edema) and exercise are advised to assist in maintaining reduced body mass index.4,57
Environmental factors contributing to xerosis
Xerotic skin due to SD is more vulnerable to damage due to friction or trauma and has increased susceptibility to contact dermatitis because of the increased penetration of substances through the impaired dermal barrier. Avoidance of environmental factors (extreme cold and heat, wind, low humidity, and ultraviolet radiation) contributing to the development and worsening of xerosis is vital in the prevention of xerosis, and suitable clothing may be worn to protect against wind, rain, and sunlight. Local environment humidity can be increased by the reduction in ambient temperature or decreasing exposure to air conditioning or heaters. Patients should avoid excessive contact with water and towel rubbing, which may damage the skin in the long term, and instead wash the legs with minimal soap, use soaps that support lower pH, and dab the skin dry.78,79
Smoking
A multivariate analysis adjusted for other risk factors showed a significant association of venous insufficiency with tobacco smoking (p < .001).80 In vivo and ex vivo studies indicate that carbon monoxide, free radicals, and tar present in cigarette smoke promote morphological and biochemical changes in the endothelium that result in decreased blood flow, and numerous clinical studies have demonstrated that smoking results in coronary vasoconstriction, increased vascular resistance, and a decrease in coronary blood flow.81,82 The importance of smoking cessation as part of the management of SD is often not fully understood because patients often see the condition as a cosmetic nuisance and are unaware of the underlying venous insufficiency.
Diabetes
The incidence of type 2 diabetes, as with CVI, increases with age.83 The metabolic abnormalities that characterize diabetes make patients more susceptible to venous diseases as they result in inflammation and vasoconstriction.84 Data derived from a quantitative survey reported that more than half of patients (53%) with CVI also had diabetes.85 Adequate glycemic control in this patient population to reduce the risk of venous disease and infection is important.
Pharmacologic treatment options
1. Skin care and emollients
For general skin care, the use of gentle non-soap cleansers (preferably without artificial fragrances or colors) and barrier preparations are advised.1 Long-term topical treatment of chronic SD involves the use of bland topical emollients to maximize epidermal moisture, reduce xerosis and pruritus, and assist in restoring skin barrier function.1,4,54,78 The choice of the ideal moisturizer may differ depending on patient preference; however, plain white petrolatum is frequently used because it is inexpensive and effective and does not contain any contact sensitizers.73,78 The moisturizer chosen should contain a humectant such as lactic acid, glycerol or urea to retain or attract water, a lipid to serve as a waterproof barrier to prevent the evaporation of water, and a keratolytic such as ammonium lactate, which may improve efficacy by normalizing desquamation.78 Although these emollients and moisturizers contain beneficial ingredients, they may also contain molecules with a sensitizing or irritating potential that may result in further damage to the skin barrier with subsequent worsening of inflammation.86 These ingredients usually have no effect on normal skin; however, SD results in skin damage and subsequent allergic sensitization.86
2. Topical therapies
Topical therapies include certain dressings, ointments, creams, lotions, and gels. The vehicle through which any active ingredients are delivered plays an important role in absorption and can improve its efficacy. Generally, ointments are more effective than creams because of their emollient action and occlusive effect, which increase absorption. In addition, ointments contain fewer preservatives and therefore have a lower potential for irritant and allergic reactions. Wet wraps and application under occlusion may be used to enhance the absorption of topical treatments such as corticosteroids.73–75
3. Topical corticosteroids
Research on the treatment of SD, including the use of topical corticosteroids (TCSs) in SD, is lacking.1,87 However, one RCT specifically evaluated the use of TCSs for the treatment of SD in which steroid-treated patients showed statistical improvement in the primary clinical endpoints in terms of erythema (p < .05) and petechiae (p < .05) versus vehicle-treated patients. Similarly, there was a statistically significant improvement in the Dermatology Life Quality Index (DLQI) compared to baseline on visit day 28 (p < .001).87
Medium- to high-potency TCSs are used to reduce inflammation during the acute phase of treatment and can also be used to relieve pruritus.1,4 A decrease in inflammation minimizes subsequent damage to venous walls and valves.43 For maintenance therapy, the use of a low- to medium-potency TCS is usually advised.73 Corticosteroids perform their function by means of vasoconstriction and subsequent decrease in the number of inflammatory cytokines and immune cells, including T lymphocytes, monocytes, dendritic cells, and their precursors, being delivered to the upper dermis.88 TCSs also inhibit phospholipase A2, which ultimately decreases the production of prostaglandins and leukotrienes.88
Long-term use of TCSs (especially high-potency TCSs) is restricted to avoid cutaneous atrophy, tachyphylaxis, and hypersensitivity, which may be immediate or non-immediate (non-immediate hypersensitivity is more common and includes allergic contact dermatitis).89 Other side effects include purpura, telangiectasias, focal hypertrichosis, and acneiform/rosacea-like eruptions.73,89,90 In addition, the use of high- and very high-potency agents can potentially result in systemic side effects such as hypothalamic-pituitary-adrenal axis suppression.89
Topical calcineurin inhibitors
Topical calcineurin inhibitors such as tacrolimus are approved for use in treating AD but not SD. They are effective in many steroid-responsive dermatoses and do not have the risk of skin atrophy or tachyphylaxis as with the use of TCS.91,92 A Cochrane meta-analysis of 14 RCTs comparing TCIs to various potencies of TCSs reported TCIs to be more effective than TCSs in the treatment of certain inflammatory dermatoses; however, the use of TCIs was associated with a higher incidence of side effects versus TCSs.93 TCIs are associated with a burning sensation upon application and require patient education due to a boxed warning for rare cases of malignancy (eg, skin cancer and lymphoma).73,90 This drug class has anti-inflammatory activity due to a suppression of the synthesis and release of pro-inflammatory cytokines, including type 1 and type 2 helper cells; interleukin-2, -3, -4, and -5; interferon-γ and tumor necrosis factor-α.91
PDE4 inhibitors
Overexpression and subsequent overactivity of PDE4, a cyclic adenosine monophosphate intracellular nonreceptor enzyme, regulates intracellular cyclic adenosine monophosphate levels, which increases the production of inflammatory cytokines which play a role in perpetuating skin barrier defects and dermal inflammation.90,94 Targeting PDE4 is an effective strategy for treating several inflammatory conditions, including atopic dermatitis, psoriasis, psoriatic arthritis, and inflammatory airway diseases, and may provide an additional approach to preventing SD-related complications and progression.90,94,95 Treatment options that limit inflammation or decrease factors leading to inflammation are advised to remedy SD-related symptoms.35
Crisaborole ointment, 2%, a nonsteroidal PDE4 inhibitor approved for the treatment of mild-to-moderate AD in multiple countries, has not been approved for use in SD.96 Other examples of PDE4 inhibitors are roflumilast, approved for chronic obstructive pulmonary disease (COPD) and plaque psoriasis, and apremilast, approved for the treatment of plaque psoriasis.94 Crisaborole does not cause skin atrophy and is rapidly metabolized to inactive metabolites that have no effect on cytokine release or PDE4 activity, limiting systemic exposure and reducing the risk of adverse effects. A topical PDE4 inhibitor could provide targeted inhibition of inflammation observed in skin diseases while avoiding the unwanted side effects associated with other topical therapies.90 There is currently a randomized, double-blind, vehicle-controlled, parallel-group, proof-of-concept phase 2a trial (ClinicalTrials.gov: NCT04091087) in adult patients with SD without active skin ulceration. This trial will evaluate and compare the efficacy and safety of crisaborole versus vehicle in these patients.97,98
Systemic treatment
Although several oral treatments have shown benefit in the treatment of SD-related symptoms, none are currently approved for use in SD by the US Food and Drug Administration or the European Medicines Agency. Other systemic therapies such as disease-modifying antirheumatic drugs (eg, methotrexate) as well as certain immunosuppressive therapies (eg, cyclosporin, azathioprine, and mycophenolate mofetil) with known anti-inflammatory properties represent additional systemic treatment options that have shown efficacy in eczema and require further investigation in patients with SD.99
1. Janus kinase inhibitors
Numerous chronic inflammatory skin diseases are associated with the release of proinflammatory cytokines, which act via the intracellular Janus kinase signal transducer and activator of transcription (JAK-STAT) pathway.100 In a phase 2a study, application of delgocitinib in patients with chronic hand eczema resulted in significant improvement according to the Physician Global Assessment of disease severity in 46% of the patients compared to 15% with placebo. In addition, the application was found to be well tolerated.101 Although there have been no such studies conducted thus far in patients with SD, numerous additional studies are anticipated to evaluate the role of these agents.100,102–106
2. Flavonoids
In the CVI setting, edema may improve with use of flavonoids (also known as venoactive drugs or phlebotonics), which reduce capillary permeability, increase venous tone, improve lymphatic drainage while reducing blood viscosity, and decrease the release of inflammatory mediators.1,107 Flavonoids affect many biological activities, and their use may be beneficial or detrimental depending on the patient’s clinical circumstances. In terms of tolerability, venoactive drugs have drug-specific adverse events; however, gastrointestinal (GI) tolerability seems to be the most common problem within this drug class, including adverse events such as epigastric discomfort, vomiting, and constipation.107,108 Further studies are needed to support long-term use of these agents.107
Micronized purified flavonoid fraction (MPFF) has shown benefit throughout all the stages of vascular disease progression. During the early stages of CVI, it may be used to prevent disease progression. MPFF has been shown to reduce periprocedural pain and bleeding and improve symptoms associated with vascular insufficiency when patients require interventional procedures. It may also be used as an adjunct to increase the healing rate of venous ulcers.109 In addition, MPFF has been shown to be more potent than other venoactive drugs in the reduction of ankle edema.110 In terms of tolerability, MPFF has been found to be well tolerated, with adverse GI effects being the most common.111
3. Hydroxyethylrutoside
Hydroxyethylrutoside (HR) is a standardized mixture of semisynthetic flavonoids and can be utilized to relieve symptoms of CVI, including pain, cramps, and heavy legs. However, further research is required before routine use can be recommended.1 In a meta-analysis of 15 studies evaluating the efficacy and tolerability of HR in patients with CVI, HR was found to significantly reduce pain, heavy legs, and cramps versus placebo. It appears to be beneficial for CVI because of its ability to inhibit capillary filtration by reducing microvascular permeability, improving microcirculation, and reducing edema. The adverse effects reported were minor, with no significant difference between the HR and placebo groups.112
4. Pentoxifylline
Pentoxifylline is a vasoactive agent that improves blood flow by reducing blood viscosity. It reduces inflammation by abrogating cytokine-mediated neutrophil activation and increases the healing rate of venous ulcers with or without compression therapy.113,114 It is currently used off-label for the treatment of venous ulcers. In patients affected by CVI, pentoxifylline (400 mg, 3 times daily) may improve tissue perfusion by enhancing blood flow and can alleviate ischemic pain.114 The most common adverse effects are nausea and vomiting, abdominal discomfort, diarrhea, headache, flushing, tachycardia, and hypertension, as well as hypotension.114
5. Oral corticosteroids
Oral corticosteroids, which reduce inflammation and pruritus, are also used for short-term treatment.115 However, caution is advised given that corticosteroids have the potential to cause fluid retention, which may cause or precipitate edema of the lower extremities. In addition, long-term use is associated with a greater potential for systemic adverse effects such as osteoporosis, metabolic adverse effects, GI bleeding, and increased risk of infections as well as cardiovascular and neuropsychiatric adverse effects and should be avoided.115
6. Diuretics
Diuretics reduce swelling and pain by drawing excess fluid from the body through the kidneys. Long-term use should be avoided because of side effects such as dehydration, which may lead to kidney damage. In addition, more frequent urination may be inconvenient.116,117 Finally, these drugs do not address the underlying pathology of SD.
7. Acetylsalicylic acid
Acetylsalicylic acid increases blood flow and suppresses inflammation which may improve SD-related symptoms. It has also been found to help heal venous leg ulcers and reduces the frequency of ulcer recurrence. In 1 RCT, daily administration of acetylsalicylic acid (300 mg) in combination with compression bandages over a 5-month period had a shorter average healing time of venous leg ulcers (VLUs) compared to compression alone (12 weeks vs 22 weeks) and the average time for recurrence was longer (39 days vs 16.3 days) compared to the compression group. However, the sample size for this trial was small, and evidence for the effectiveness of acetylsalicylic acid on ulcer healing and recurrence in high-quality RCTs is currently lacking.118,119 More importantly, this trial was not designed to focus on SD; therefore, caution is advised because the inference of effectiveness in SD is not trivial. The use of acetylsalicylic acid can be problematic because of its association with certain adverse effects, especially if used long-term. Aside from heartburn and increased abdominal pain, the use of acetylsalicylic acid is also associated with more serious complications, including GI or cerebral bleeding.120
8. Antihistamines
Antihistamines can be used in an attempt to relieve pruritus, but responses are poor because pruritus associated with SD is thought to be nonhistaminergic.47,52
9. Herbal supplements
Although herbal supplements are used to treat SD, many are not approved by a regulatory body for use, and they vary in quality, efficacy, and safety.102 Certain herbal supplements may be used to manage swelling, and two RCTs have identified short-term improvement in CVI with herbal horse chestnut seed extract (HCSE) containing aescin and flavonoids (glycosides of quercetin and kaempferol).103,104 HCSE and aescin reduce inflammation and edema by counteracting adenosine triphosphate reduction and the subsequent increased activity of phospholipase A2, reducing the release of inflammatory mediators.103,104 Furthermore, HCSE and aescin increase the production of prostaglandin F2, resulting in an increase in tension in vein walls that increases blood velocity and venous outflow, improving microcirculation.104,105 According to a Cochrane review, evidence suggests that HCSE is efficacious and safe for short-term use in CVI; however, there is insufficient evidence to recommend long-term use. Adverse effects included infrequent reports of mild gastrointestinal complaints, dizziness, nausea, headache, and pruritus.106
Interventional treatment options
Interventional treatment options include surgical as well as other less invasive venous procedures. A variety of surgical methods are available to correct the underlying cause of reflux and increased venous pressure associated with CVI, including ligation and stripping, perforator surgery, and valve reconstruction; however, newer, minimally invasive venous procedures such as endovenous thermal ablation, ambulatory phlebotomy, and sclerotherapy are often preferred. These newer procedures have advantages over the more invasive surgical procedures, including less postoperative pain, lower incidence of complications, faster recovery, and lower costs.1,2 Several studies have noted a marked improvement in SD-related symptoms and a lower recurrence rate associated with the use of interventional treatment options versus more conservative treatment options such as compression therapy, substantiating the importance of addressing underlying CVI.2,121–123 However, the recurrence of SD and SD-related complications after the resolution of symptoms remain a problem because CVI is a chronic disorder.2,124 In addition, other health-related conditions and risk factors which may have contributed to the development of CVI may still be present. Treatment options depend on the disease severity as well as anatomical considerations such as pre-existing tissue damage, in which case procedures that allow access to incompetent veins and/or valves from a site that is distant from the affected tissue are considered.2
1. Treatment of skin discoloration
Skin discoloration is very hard to treat successfully and typically does not resolve even when the underlying CVI is well controlled; however, some reports have noted that improvements can be achieved with an intense pulsed light source. Patients bothered by the cosmetic appearance will often use concealing cosmetic products.1
Pulsed light or laser treatment
Cutaneous hyperpigmentation often persists even if the CVI is treated; although responses are often poor, noncoherent intense pulsed light or laser treatments do represent an approach to facilitating the removal of hyperpigmentation.1
Red-light therapy
Used for treating inflammation and hyperpigmentation of the skin, this form of light therapy delivers light of a lower intensity and a lower level of absorption to the skin versus pulsed light. Red-light therapy is, however, gentler on the skin. Red-light therapy is considered safe, with few reports of burns and blistering. There is a potential risk of damage to the eyes, and proper eye protection is advised during therapy.98
2. Surgery
When conservative measures do not achieve adequate improvement; patients with persistent discomfort, disability, and nonhealing venous ulcers due to CVI may require invasive surgical management.2 Although the risk of recurrence of venous ulcers after surgery remains, it is lower than that of more conservative treatments such as the use of compression stockings or bandages.2,121–123,125
Surgical techniques include vein stripping and ligation, to improve venous hemodynamics and provide symptomatic relief.2 Ulcer recurrence rate has been found to be improved in patients with CVI, demonstrating a lower rate of recurrence when used together with compression therapy versus compression therapy alone (12% vs 28%).122 Vein stripping and ligation are generally well tolerated; however, as with most surgical procedures, there is a risk for infection at the surgical site, DVT and irritation of the nerves that traverse along the stripped veins. Pain at the incision sites is common; however, this is usually minimal.1,126,127
Perforator surgery ligates incompetent perforator veins by gaining access from a site that is distal to the affected skin and is associated with high rates of ulcer healing (~90% at 3–12 months) and low rates of recurrence (<30% at 2 years).2,128,129 Subfascial endoscopic perforator surgery is contraindicated in patients with lower extremity edema and obesity and is generally avoided in older patients.130 Complications include hematoma, cellulitis, wound dehiscence or seroma, and skin nerve injury.131
Valve reconstruction is used in advanced cases, providing competency in ~30%–40% of cases and a cumulative ulcer free recurrence of ~50% at 36 months. Potential complications include bleeding, DVT, pulmonary embolism (PE), seroma, and an increased risk of wound infections. This procedure is more expensive compared with other surgical procedures.2,132
3. Minimally invasive procedures
Open surgical techniques have largely been replaced by minimally invasive procedures such as thermal ablation, sclerotherapy, phlebectomy, and VenaSealTM (Covidien LLC, Morrisville, NC, United States).
Thermal ablation
Thermal ablation is performed on incompetent superficial veins via laser (endovenous laser therapy [EVLT]) or radiofrequency ablation (RFA), which induce fibrosis or thrombosis of the refluxed veins (Figure 4)1,2 Thermal ablation is now considered the gold standard interventional treatment in the management of CVI according to guidance documents and recent data.2,133,134 Increased efficacy and the reduced invasiveness of thermal ablation makes it a favored intervention.135,136 Cost varies depending on the size of the area requiring treatment.1 This technique is associated with less procedural pain and faster improvement in symptom score and QoL as well as fewer adverse events and complications versus invasive surgical procedures.1 Postoperative complications may include thrombophlebitis, thermal skin injury, bruising, hyperpigmentation, paresthesia, wound infection, and hematomas. Lower recurrence rates versus classical surgery have also been reported.2,134
_and_after_(B)_endovenous_thermal_ablation._Reproduced_with_permi)
Sclerotherapy
Sclerotherapy is a procedure involving the injection of liquid or foam chemical agents (sclerosants) into dilated veins, including major refluxing trunks or tributary varicosities, venules, or telangiectasias, which cause scarring in the veins so that they can no longer carry blood. The body subsequently absorbs the scarred veins and blood returns to the heart through other veins.2,19,134 This is an off-label use in the USA, although it has demonstrated efficacy.1 There are certain limitations to this form of therapy, including dilution disparities, its progressive inactivation, and its inaccuracy of the desired effect once injected in the blood vessel.19 Sclerotherapy has a relatively faster recovery period, is associated with less pain, and is less expensive compared to the surgical procedures available or thermal ablation.134 However, additional or repeated treatment is needed more often than with certain surgical procedures. Potential adverse effects include skin necrosis, hyperpigmentation, and allergic reactions. Complications such as DVT or PE may also occur.2,134
Phlebectomy
Ambulatory phlebectomy is used in conjunction with other venous procedures and involves the removal of varicose veins through 2- to 3-mm incisions in the skin overlying the veins.1 In a study comparing the recurrence rate for venous incompetence, phlebectomy was associated with a lower recurrence rate versus liquid sclerotherapy plus compression at 1 and 2 years of follow-up.137 Potential postoperative complications include wound infection, keloid formation, hypo- or hyperpigmentation, DVT, PE, and nerve damage.138
VenaSealTM
VenaSealTM is a device used in combination with cyanoacrylate glue to occlude the vein lumen of incompetent truncal veins in patients with varicose veins or more advanced chronic venous diseases, associated with anatomical success (veins completely obliterated) within 48 hours of the procedure.139 Adverse events were mostly mild and self-limiting, with phlebitis being the most common (occurring in 16% of patients).139–141 Contraindications include patients with a history of hypersensitivity, acute venous thromboembolism, and sepsis.139 Although the success rates and safety profile of this procedure was found to be favorable, this technique is associated with high rates of recurrence, and further studies are needed to evaluate long-term outcomes.139,142
Emerging therapies
Given its role in the pathogenesis of SD, inflammation represents a logical target for the development of new therapeutic options.95
1. Diode laser
Diode laser therapy has been used to accelerate wound healing by treating the underlying venous insufficiency as shown in a retrospective study (n = 287) whereby patients underwent surgery to treat superficial venous insufficiency with a diode laser. There were 358 GSVs and 84 small saphenous veins treated during the study. The total occlusion rates after 12 months of surgery were 94.4% in the GSVs and 96.4% in the small saphenous veins. This proved to be a safe and effective treatment, with low rates of complications.143
2. Physiotherapy
The calf muscle pump, of which the ankle joint is the main component, is essential in venous return of blood from the lower extremities to the heart. Effective functioning of the calf muscle pump relies on dorsiflexion and plantar flexion of the ankle, and therefore a lack of ankle mobility increases the severity of edema formation and venous reflux in patients with CVI. The presence of any abnormality in pump function of calf muscle plays a significant role in the development of CVI. In patients with CVI, progressive exercise programs have been used to rehabilitate the muscle pump function and improve symptoms.144
Treatment of SD Complications
Complications associated with SD include cellulitis, abscesses, and superinfections such as ecthyma, as well as contact dermatitis, autoeczematization, and disease progression that may lead to venous ulcers (CEAP classes C5 and C6), osteomyelitis, and acute LDS, all of which require effective and timely management.14,154 There are various conservative, medicinal, and interventional treatment options available to manage the underlying CVI.1,2 If secondary, bacterial infections are present in skin affected by SD (eg, cellulitis, abscess formation, skin ulcer infection) treatment with debridement and drainage, as well as topically or systemically administered antibiotics may be considered, depending on the type of infection.4 Autoeczematization (“id reaction”) may complicate SD with acute, generalized, extremely pruritic, erythematous or papulovesicular dermatitis distal to SD lesions.149 Treatment includes wet wraps or dressings for weepy eczematous plaques, potassium permanganate soaks for localized oozing and infected areas, potent systemic steroids, or topical corticosteroids (TCSs) and/or an oral sedating antihistamine at night.149,150 Acute LDS is an inflammatory condition characterized by subcutaneous fibrosis and hardening of the skin on the lower legs, resulting from CVI.26,31,155 The recommended management in this case includes compression combined with oxandrolone, stanozolol (reduce pain and dermal thickness), pentoxifylline, corticosteroids, phlebotonic drugs, horse chestnut seed extract (HCSE), capsaicin, and/or emollients26,152,153 (Table 2).
Follow-up
To improve adherence, the establishment of an honest and trustworthy relationship between patients and health care professionals is crucial, along with adequate education and counseling.1,156 SD is a chronic condition that requires the patient’s progress to be monitored during regularly scheduled follow-up visits. Due to the progressive nature of SD, symptoms such as pain, leg heaviness, pruritus, and edema may worsen with time.1,4,7 Consequently, the patient’s therapeutic regimen may need to be adjusted to provide adequate relief and prevent the further worsening of symptoms. In addition, these visits are essential to monitoring the patient’s progress and motivating and educating them.156
SD exacerbations should be closely monitored via office visits and patient observation for the development of complications (eg, infection and ulcers). A follow-up with a dermatologist or general physician may also be required. Also, patients should be informed that any improvement they experience is a direct result of therapy and that without it, their condition will deteriorate. When patients have good control and an adequate understanding of SD and CVI, follow-ups will become less frequent as patients become more comfortable managing their SD themselves when their symptoms are under control.
Conclusions
SD is a chronic, relapsing condition associated with troublesome and at times debilitating symptoms including pruritus, edema, and heavy or aching legs as well as pain that substantially affects patient QoL. Cosmetic concerns including skin discoloration and venous ulcers may result in embarrassment and social isolation. SD is often misdiagnosed, misunderstood, and managed incorrectly, resulting in avoidable worsening symptoms and disease progression as well as secondary complications. However, even with timely, accurate diagnosis and appropriate management, SD requires constant management and follow-up.
Initial management involves conservative approaches to reducing symptoms and preventing secondary complications and disease progression, followed by more invasive interventions in more severe cases. There remains an unmet need for additional treatment options. To treat the patient optimally, the pathogenesis of SD and the etiopathological relationship between CVI and SD needs to be more fully evaluated. In addition, the treatment and management of risk factors of CVI and secondary complications forms an important part of these patients’ therapeutic plans. Only once all these factors are considered can SD be optimally managed.
Acknowledgments
Editorial and medical writing support, under the guidance of the authors, was provided by David Gibson, PhD, CMPP, Chantell Hayward, PharmD, and Paul Sobol, PhD, at ApotheCom, San Francisco, CA, USA, and was funded by Pfizer Inc., New York, NY, USA, in accordance with Good Publication Practice guidelines (GPP 2022) guidelines (Ann Intern Med. 2022; 10.7326/M22-1460).
Conflicts of Interest
GSF and BV are employees and shareholders of Pfizer Inc. HL-T served as a consultant for AbbVie, NextScience, Novartis and Pfizer Inc. RN had no conflicts of interest to declare.
IO served as a speaker for Pfizer Inc. and AbbVie. GW served as a speaker, advisory board member and consultant for Janssen and La Roche-Posay and has served as a speaker for Pfizer Inc., Novartis, AbbVie, Boehringer Ingelheim, Eli Lilly and Company, LEO Pharma, and Sanofi outside the submitted work.
Funding
This study was sponsored by Pfizer.