Introduction
Atopic dermatitis (AD) is a chronic, relapsing inflammatory skin disorder characterized by cycles of intermittent exacerbations interspersed with periods of relative control.1 Managing AD can be difficult due to its dynamicity: signs and symptoms of AD wax and wane over the course of years, months, and even days. Yet, many of the validated instruments used to evaluate AD control heavily rely on visual snapshots that reveal only a piece of the larger disease progression.2 While the clinician-assessed measures are efficient in providing a succinct, visual characterization of AD in clinic visits, unfortunately, many of these tools, such as the often-used Investigator Global Assessment (IGA)3 and Eczema Area Severity Index (EASI),4 lack representation of a comprehensive overview of health-related quality of life (QoL) measures that are intricately tied to patient satisfaction.5,6 Variables factored into physician-assessed clinical severity may be discordant with patient-reported outcomes (PROs).7 Thus, the increased incorporation of PROs in randomized clinical trials reflects clinicians’ understanding that successful AD control relies on treatments that effectively manage clinical signs of AD in addition to patient-reported symptoms, such as pruritus, pain, and sleep disturbances—all factors intricately tied to patient burden of AD.8–10
Patient-reported outcomes measures (PROMs) are increasingly acknowledged as important instruments by physicians, regulators, and pharmaceutical companies for their importance in incorporating patient-centered data in clinical trials. In fact, they are often incorporated as primary or secondary endpoints in randomized controlled trials (RCTs). The increasing emphasis on integrating PROs in AD clinical trials may improve patient adherence to treatment by focusing on patient needs and preferences that matter most in considering treatment options in the real-world.11 The chronic, relapsing nature of AD lends itself to the prolonged use of conventional treatment options—ranging from topical corticosteroids, calcineurin inhibitors, systemic immunomodulatory medications, and biologic agents. While these treatments may be effective, they are accompanied by potential side effects that may make them undesirable for certain patients.12,13 Thus, complementary and alternative (CAM) approaches used in adjunct to conventional AD treatment may provide additional relief for patients. CAM therapies are often flexibly integrated into a patient’s lifestyle without temporal restrictions that limit many traditional AD therapies.14 Despite the widespread use of CAM therapies by AD patients, there is a lack of RCTs that assess the efficacy of integrative approaches with PROMs.15 Thus, this review aims to evaluate CAM therapies through RCTs that used PROMs in AD management.
Materials and Methods
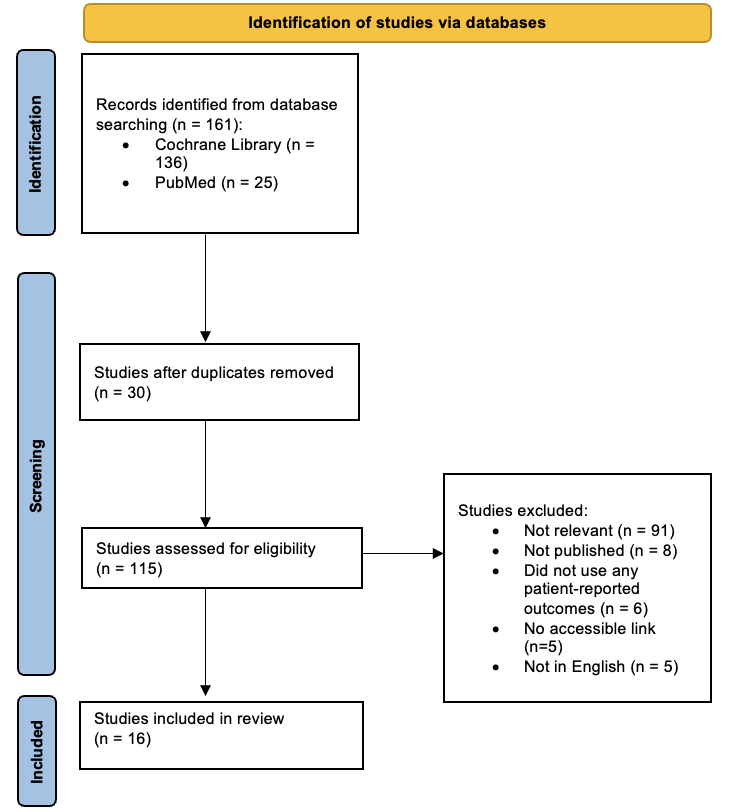
Following the guidelines of PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses),16 a search of PubMed and the Cochrane Central Register of Controlled Trials was conducted from March 2015 to March 2024 to identify all RCTs investigating CAM approaches for AD management that used at least one PROM as a primary or secondary endpoint (Figure 1). Medical subject headings (MeSH) queried in the systematic search were atopic dermatitis, acupuncture, acupressure, sunflower, coconut, primrose, massage, hypnosis, bath, and tea. The PROMs that met inclusion criteria were the following: Atopic Dermatitis Control Tool (ADCT),17 Patient-Oriented Eczema Measure (POEM),18 Patient-Oriented SCORing of Atopic Dermatitis (PO-SCORAD),19 Recap of Atopic Eczema (RECAP),20 Peak Pruritus Numerical Rating Score (PP-NRS),21 Dermatology Life Quality Index (DLQI),22 Short Form 12 (SF-12),23 Visual Analog Scale (VAS) (pruritus, sleep disturbances/insomnia, etc).24

RCTs that met inclusion and exclusion criteria were limited to studies published in the English language and those composed of at least ten or more human subjects. Trials excluded were RCTs that did not directly investigate CAM therapy as a primary intervention, published final outcomes, incorporated PROMs in study outcomes, lacked an accessible link, and published in a non-English language. A manual review of the titles and abstracts was conducted, and full texts of manuscripts were reviewed to determine eligibility.
Results
A total of 161 articles were identified in the initial search from Cochrane Central Register of Controlled Trials (n = 136) and PubMed (n = 25). After 30 duplicate trials were removed, 115 studies were assessed for eligibility. The exclusion criteria were the following: irrelevance in directly investigating CAM therapy as a primary AD intervention (n = 91), did not progress to publication (n = 8), lacked at least one PROM to evaluate clinical efficacy in AD intervention (n = 6), lacked an accessible link (n = 5), and were not in the English language (n = 5). Sixteen trials met inclusion criteria and were evaluated in this review.
Acupuncture
A cornerstone of traditional Chinese medicine, acupuncture is increasingly recognized as a viable alternative therapy for managing AD. By inserting fine needles into specific points on the body, acupuncture promotes healing by ostensibly restoring balance of “qi”—the body’s vital energy.25 In fact, acupuncture is shown to demonstrate immunomodulatory effects in reducing itch intensity by dampening allergen-induced basophil activation.26 A commonly used acupuncture point called Large Intestine-11 (LI-11) reduced not only skin inflammation but also ameliorated serotonergic itch via blockade of 5-HT2 and 5-HT7 in murine models with induced AD skin.27 Further, acupuncture in LI-11 attenuated scratching behavior, offering potential in breaking the itch-scratch cycle that perpetuates inflammation in AD.28,29
Three RCTs on acupuncture met inclusion criteria. Park et al (n = 36) found that there were no significant differences across all indices in true acupuncture (TA) and sham acupuncture (SA) groups. While the TA group maintained SCORAD and EASI scores for at least 4 weeks during follow-up, there was no difference in PROMs–POEM, DLQI, VAS (pruritus), and VAS (insomnia). The authors hypothesized that acupuncture works through specific and non-specific effects, and the expectancy of treatment primarily responsible for the non-specific benefits of acupuncture was fulfilled by the sham treatment. However, the effects of acupuncture were sustained in TA during treatment and follow-up period. Compared to SA, TA SCORAD score substantially decreased 2 weeks after intervention and continually improved during the follow-up period (both p < 0.0001). The study was limited in its small sample size along with the patients’ baseline AD clinical severity (mild-to-moderate), requiring further RCTs to elucidate acupuncture treatment in AD.30
Rotter et al conducted a three-armed RCT that compared acupuncture to osteopathic medicine and control. Acupuncture demonstrated a clinically relevant difference in VAS itching between control (p < 0.05) and decreased topical corticosteroid (TCS) use was noted. Interestingly, upon health economics analysis on the cost-effectiveness of acupuncture treatment defined by AD-related total costs (number of sick days, impaired work hours, and utilization of healthcare related to AD), acupuncture was not shown to be superior to osteopathic medicine nor control. While SCORAD or EASI revealed no differences, clinical improvement in itch supports acupuncture as an adjuvant therapy in managing AD.31
While the SCORAD between TA and SA was not significant (p = 0.089), Abad-Constantino similarly found that both TA and SA acupuncture groups showed reduction in VAS (pruritus) scores along with decreased TCS use. The true acupuncture group reported greater reductions (p = 0.009) sustained after the end of treatment, suggesting that acupuncture may serve as an effective adjuvant modality in controlling pruritus. The comparable efficacy of TA to SA may be attributed to the acupuncture needle stimulating the cutaneous A-gamma or C fibers that subsequently depletes the neurotransmitters mediating pruritus thus attenuating tachyphylaxis (p < 0.001).32 Moreover, the DLQI and CDLQI scores also revealed greater improvement in QoL in the TA group.33
Acupuncture has been used to manage AD, and its efficacy has been demonstrated in multiple pruritic dermatoses, including prurigo nodularis,34 uremic pruritus,35 and neuropathic pruritus.36 Pruritus is one of the most challenging AD burdens, impacting patients’ QoL with associations with anxiety, depression, difficulty concentrating, and decrease in sexual desire and function.37 Thus, the three RCTs demonstrating the efficacy of acupuncture in alleviating pruritus along with AD severity may illustrate acupuncture as a promising adjunct treatment for patients seeking integrative approaches in achieving AD control.
Topical Oils
The history of using natural oils for broken skin dates back at least centuries, with various cultures incorporating plant-based oils into traditional remedies for skin conditions.38 Ancient civilizations utilized oils for their moisturizing and soothing properties. It follows then that natural oils have been a popular CAM approach for AD, rooted in ancient practices that have been continually studied into the modern era.39 Of the many topical oils, two RCTs on primrose oil, sunflower seed oil, and coconut oil met inclusion criteria.
Sunflower Seed Oil and Coconut Oil
Sunflower seed (Helianthus annus) oil is rich in linoleic acid, which has been shown to have anti-inflammatory properties by serving as a precursor for prostaglandin E2 (PGE2) that drives cutaneous inflammation.40 Further, sunflower oleodistillates (SOD) serve as a potent activator of peroxisome proliferator-activated receptor-α (PPAR-α) that improves skin barrier by stimulating keratinocyte differentiation; in fact, Dubuqoy et al suggested that 2% SOD may demonstrate similar clinical efficacy to a mid-potency topical corticosteroid.41
Coconut (Cocos nucifera) oil is another botanical oil used as a CAM modality for AD management, thought to have both emollient and antimicrobial properties.42 In a study that compared coconut oil to mineral oil in children with AD, coconut oil was found to be superior to mineral oil with a 68% and 38% reduction in SCORAD respectively (p < 0.001).43 Further, the refining process of virgin coconut oil (VCO) leaves behind only a tiny fraction of coconut protein, which appears to eliminate most of the likely candidates for triggering allergic reactions, rendering VCO a safe and efficacious option.44
Nadora et al performed an RCT that compared isosorbide diesters (IDEAS, 4% isosorbide dicaprylate and 4% isosorbide disunflowerseedate) in sunflower seed oil and coconut oil with the control vehicle of 0.1% colloidal oatmeal. The IDEAs group reported a 65.6% improvement in their VAS (pruritus) score compared to the 43.8% reported in the vehicle group (p = 0.013). Moreover, the relative abundance of Staphylococcus aureus was decreased in the IDEAS group compared with the no change in the vehicle group (p = 0.044). The IDEAS group further noted improved AD clinical severity indicated by 56.5% of patients in IDEAS versus 25% in placebo control achieving EASI-75 scores by week 4 (p = 0.07).45
Evening primrose oil
Evening primrose oil (EPO), derived from Oenothera biennis seeds, has garnered attention for its rich gamma-linolenic acid (GLA) content, a subtype of omega-6 fatty acid that is anti-inflammatory.46 EPO has also been shown to inhibit the production of pro-inflammatory metabolites in the arachidonic acid pathway by upregulating PGE1, decreasing acute inflammation.47 Chung et al conducted a RCT that compared EPO to soybean oil. While there was no significant difference in VAS (pruritus) scores, differential improvement of EASI depending on age was noted with EPO improving EASI scores in under age 12 (p = 0.002) but not in over age 12 (p = 0.481).48
The improvements in AD clinical severity along with varying degrees of itch underscores that, while generally correlated, clinician-assessed outcomes may not always be concordant with patient-reported symptoms. With Nadora et al demonstrating itch reduction with sunflower seed oil and coconut oil (p = 0.013) use along with Chung et al finding improvements in AD severity in patients under age 12,45,48 these topical oils can be easily integrated into patients’ standard AD management, especially to optimize care for patients with contraindications to other therapies, including pediatric patients, geriatric patients, and patients with numerous comorbidities. While the use of topical oils shows promise in AD management, further studies must be conducted to better characterize their benefits in integrative AD management.
Stress and Skin: Mind-Body Therapies
The skin not only responds to external stress but also reflects internal stressors impacting the body. When stress is perceived, the hypothalamic-pituitary-adrenal axis activates downstream expression of cortisol, which may decrease the immune response in chronic stress. Moreover, perceived stress may upregulate pruritogenic agents in the nervous system to lower the itch threshold, exacerbating the itch-scratch cycle that is the hallmark of AD.49 Thus, mind-body therapies, such as hypnosis, biofeedback, massage, and meditation techniques have emerged to better combat the impact of stress on AD.50
Hypnosis, Intermittent Fasting with Diet Changes, and Exercise
Hypnosis is a state of altered consciousness that can impact the perception of reality and physiologic responses.51 While the exact mechanism is yet to be uncovered, hypnosis has shown to modulate activation of specific regions of the brain through regional cerebral blood flow.52 Hypnosis has been used for a wide range of dermatologic conditions via positive suggestions, but RCTs that demonstrate clinical efficacy of hypnosis in AD are sparse.
Rotter et al designed a RCT (n = 17) that compared hypnotherapy group program (HTP), intermittent fasting with diet adjustment group program (IFDP), and an exercise program that served as a control. Due to COVID-19, recruitment was limited and the in-person HTP sessions had to be flexibly readjusted as self-administered HTP. Despite the circumstances, HTP (n = 6) showed improvement in VAS pruritus, VAS sleep disturbances, DLQI, SF-6, and SF-12, although the improvement was not always consistent through the 24 week mark.53 While Rotter et al were limited in study scale due to the pandemic, they uncovered promising results in HTP that mirrored a RCT conducted by Stewart et al, which demonstrated improvements in itching, sleep disturbances, and mood in severe, recalcitrant AD up to two years.54 Overall, the study elucidates the potential of hypnotherapy as an adjuvant mind-body therapy, but further large-scale studies must be conducted.
Mother-performed Infantile Massage
Mother-performed infantile massage (MPIM) has been proven to not only reduce the relapse rates of AD but also provide mental health benefits to the caretaker providing the massage.55 In a three-armed RCT in full-term infants (AD infants with MPIM, AD infant control, and healthy infant control), Lin et al. reported improvement in EASI (p < 0.001) and relapse rate (p < 0.01) in AD infants with MPIM vs. AD infants control. Further, AD infants that received MPIM showed improvement in IDQOL (p < 0.001).56 Thus, given the ease and flexibility of performing MPIM, MPIM has great potential to serve as an adjuvant treatment that can be performed when applying emollients as part of the standard AD therapy.
Mind-body therapies have demonstrated immense potential in alleviating symptoms that burden patients the most. MPIM may help mediate neuropsychiatric comorbidities, including depression, anxiety, and attention-deficit/hyperactivity disorders, that are commonly associated with pediatric AD.57 Further, MPIM may be superior to relaxation therapy in pediatric patients due to compliance, reduced peripheral vasoconstriction secondary to vagal stimulation and decreased stress, and its demonstrated effects on itch. Schachner et al conducted a landmark RCT that found improvement in the focal areas for AD measures (redness, lichenification, scaling, excoriation, and pruritus) as well as global areas for AD (scaling and excoriation) (p < 0.05), establishing MPIM as an effective approach for pediatric patients and caregivers.58 Thus, mind-body therapies may confer a bidirectional benefit by mediating the psychocutaneous interplay in AD, improving patient well-being and QoL as well as AD symptoms.
Bath Additives
Prior to the advent of modern therapeutics for AD, bath additives have been long studied for AD. In the late 19th century, Hebra recommended a frequent bathing regimen of up to three to four times daily; later, this view was challenged in the mid-20th century by Sholtz who hypothesized bathing to be harmful for AD skin.59,60 To this day, bathing regimens and additives serve as a popular integrative approach. Our search yielded four types of bath additives, consisting of tannic acid (TA), pine tar, paraffin, and emollient additives.
Tannic Acid
TA is a type of polyphenol, a class of compounds with antioxidant properties found in various plants, including grapes and Camellia sinensis.61,62 Used in traditional medicines for centuries, a study on AD murine models found that TA displayed therapeutic benefits in AD by suppressing angiogenesis and thymus and activation regulated chemokine (TARC) expression, decreasing Th2 cytokines.63 Further, TA inhibits nuclear factor kappa B (NF-κB) signaling by inducing PPAR-γ protein, subsequently decreasing inflammation that drives AD immunopathophysiology.62 In a RCT that met inclusion criteria, Takahagi et al compared TA- and placebo-bath additives with the VAS (pruritus) score as an endpoint. For both TA and placebo-bath additives, patients in the overall cohort reported an improvement in pruritus in all observed periods of the morning and afternoon. Both cohorts showed comparable efficacy in controlling pruritus, which the researchers attributed to the placebo’s vehicle effect (no TA included with sodium sulfate, malic acid, sodium glutamate, and uranine). Interestingly, when the analysis was confined to patients with mild-to-moderate AD, TA showed a significant improvement in pruritus at night compared with placebo. Considering that no contact dermatitis or serious adverse effects were noted in the RCT, TA may serve as a safe alternative to use adjuvant in mild-to-moderate patients.64
Pine Tar
Pine tar is another commonly utilized CAM modality used to treat skin conditions like AD, psoriasis, and dermatitis due to its properties of polycyclic aromatic hydrocarbons (PAHs) that exhibit anti-inflammatory effects and antiseptic effects.65 In a 3-month investigator-blinded, crossover, RCT (n = 43), Ng et al found significant improvement in measured indices: total SCORAD (p = 0.0024), objective SCORAD (p = 0.011), extent (p = 0.014), intensity (p = 0.032), pruritus (p = 0.047), POEM (p = 0.044), SA colonization status (p = 0.035), and log-transformed IgE level (p = 0.028). Specifically, improvements in the POEM scores were shown in pine-tar bathing but not the vehicle oil in both the intention to treat analysis (p = 0.004) and per protocol (p = 0.044) analysis.66
Paraffin
Paraffin provides a protective occlusive layer to prevent transepidermal water loss, which may help augment the skin barrier dysfunction in AD.67 However, one study found that simple paraffin repleted the skin’s natural moisturizing factor.68 Mixed results in literature warrant a RCT to elucidate the role of paraffin in AD management. Thus, Waked et al conducted a 12-week parallel-group, active-control, RCT (n = 52) in chronic hand eczema patients. The treatment group yielded greater improvement in SCORAD scores (28.6% versus 0.41%), and the patient-reported DLQI scores aligned with physician-assessed AD severity (60% versus 3.8%).69 While further studies are needed to better characterize the efficacy of paraffin, there is encouraging evidence that paraffin may be a cost-effective method in improving QoL measures, including itching and sleep disturbances, paralleled by improvements in AD severity.
Emollient Bath Additives
Emollient bath additives are a broad umbrella term that includes the aforementioned ingredients. Commonly prescribed in general practices for pediatric AD patients, there is a dearth in comprehensive RCTs that evaluate the emollient additives’ efficacy. Thus, the BATHE trial sought to elucidate the practical clinical benefits of AD through a multicenter, pragmatic, parallel group RCT (n = 483) in the United Kingdom with the POEM score as its primary outcome. The intervention group was provided with three commonly prescribed emollient additives: Oilatum (Glaxoine; 63% light liquid paraffin); Balneum Almirall; 85% soya oil); or Aveeno (Johnson & Johnson). After 16 weeks, POEM scores were 0.41 higher in the treatment versus control group, which was lower than the 3-point clinically important difference in the POEM scale. While emollient additives were found to confer no clinical benefits, standard AD treatment was encouraged in both groups, such as soap avoidance and leave-on emollients.70
Pine tar and paraffin were both successful in alleviating pruritus and AD severity, while the larger scale BATHE trial concluded no clinical benefits compared to standard AD management without emollient bath additives. Considering bath additives are a heterogeneous group of ingredients, further studies may help uncover clinical benefits as well as patient-reported symptoms of adjunct bath additive use.
Discussion
PROMs incorporate a unique viewpoint that has traditionally been overlooked in RCTs: the patient’s perspective. Especially in a chronic, relapsing condition like AD, PROMs are invaluable tools to integrate signs and symptoms of AD that pragmatically impact patients the most. The most assessed patient-reported symptoms were itch and sleep disturbances. In fact, itch was included as an outcome in all RCTs evaluated either as a PROM or incorporated through a non-PROM tool. Moreover, mind-body therapies demonstrate the most promising potential in alleviating PROs by improving AD-related symptoms in addition to comorbid psychiatric symptoms.
While almost half of AD patients flexibly utilize CAM approaches to manage their condition,71 due to the extensive realm of CAM that can encompass almost anything under the sun, there is a lack of comprehensive studies that thoroughly evaluate these approaches. Yet, the dearth of evidence-based knowledge does not negate its efficacy. Rather, it signals towards more studies that critically evaluate CAM modalities to increase patient options in AD management and ultimately improve AD treatment outcomes and patients’ QoL. Thus, future large-scale studies are needed to better characterize the benefits of these integrative approaches in AD management.
Disclosures
Dr. Lio reports being on the speaker’s bureau for AbbVie, Arcutis, Eli Lilly, Galderma, Hyphens Pharma, Incyte, La Roche-Posay/L’Oréal, Pfizer, Pierre-Fabre Dermatologie, Regeneron/Sanofi Genzyme, Verrica; reports consulting/advisory boards for Alphyn Biologics (stock options), AbbVie, Almirall, Amyris, Arcutis, ASLAN, Bristol-Myers Squibb, Burt’s Bees, Castle Biosciences, Codex Labs (stock options), Concerto Biosci (stock options), Dermavant, Eli Lilly, Galderma, Janssen, LEO Pharma, Lipidor, L’Oréal, Merck, Micreos, MyOR Diagnostics, Regeneron/Sanofi Genzyme, Sibel Health, Skinfix, Suneco Technologies (stock options), Theraplex, UCB, Unilever, Verdant Scientific (stock options), Verrica, Yobee Care (stock options). In addition, Dr. Lio has a patent pending for a Theraplex product with royalties paid and is a Board member and Scientific Advisory Committee Member emeritus of the National Eczema Association. Jiwon Park has no conflicts of interest or relationships to disclose.
Funding
This research received no funding.