Atopic dermatitis (AD) is a chronic, pruritic inflammatory skin condition affecting individuals of all ages, with a higher prevalence in children.1–3 Its impact on quality of life (QoL) is profound, as persistent flares contribute to anxiety, depression, sleep disruption, difficulty concentrating, and social isolation.1–3 Although the exact pathogenesis of AD remains unclear, it is recognized as a complex disorder influenced by factors such as skin barrier dysfunction, immune dysregulation, microbiome imbalance, and neuro-behavioral elements.1–3 While a range of conventional treatments exist, including topical corticosteroids (TCS), calcineurin inhibitors (TCIs), antibiotics, and immunosuppressants, many patients fail to experience a sufficient improvement in symptoms and quality of life.1,4 Additionally, concerns about medication safety have become more prominent on social media, prompting patients and families to explore the realm of complementary and alternative medicine.5
Recently the American Academy of Dermatology (AAD) and the American Academy of Allergy, Asthma, and Immunology/American College of Allergy, Asthma, and Immunology Joint Task Force (JTF) have released updated guidelines that focus on topical and systemic treatment of AD.2,3,6 In general, the evidence-based guidelines discuss avoiding exacerbating factors (allergens, triggers, irritants, etc) and encourage regular use of moisturizers.2,3 Regularly established skin care has shown to be efficacious in symptomatic relief of AD.7
Educating patients—particularly within pediatric populations—about the AD disease process and its impact on quality of life can help set more realistic expectations and inform them about the full range of available therapeutic options.8 It is also important to discuss the potential for secondary infectious complications of AD given the increased risk of skin and systemic infections caused by a compromised skin barrier, especially for those who may be hesitant about treatments.9 Therapies such as dilute bleach baths may be helpful in reducing inflammation and strengthening the skin barrier.1,10
Finally, the accuracy of the AD diagnosis should be carefully considered, as AD symptoms—especially in children—can mimic other conditions such as contact dermatitis, scabies, tinea corporis, psoriasis, and in rare cases, more serious conditions such as cutaneous T-cell lymphoma (CTCL) or secondary drug reactions to treatments.11–13
The AAD guidelines recommend using TCS, TCIs, topical PDE-4 inhibitors, and topical janus kinase inhibitors (JAKi) for mild-to-moderate AD, while the JTF guidelines disagree only on the topical JAKi use due to concerns about the boxed warning, highlighting patient fears about conventional medications.2,6 For moderate and severe AD, the guidelines recommends using biologic agents, including dupilumab and tralokinumab, and the JAKi upacitinib and abrocitinib.3 Moreover, systemic therapies such as NB-UVB phototherapy, cyclosporine, and even the use of whole body cryotherapy can be considered for AD that is not responsive to baseline or topical therapy.3,4,14–17 In-patient admission to the hospital or to an eczema day program may be another option for recalcitrant AD, especially in the situation of active flares or infection.18
While many unconventional therapies for AD have been studied and shown to be efficacious, almost all are presented without context, usually as monotherapies. A truly “integrative” approach suggests using such treatments alongside of more conventional ones, and yet the development of practical, standardized integrative guidelines remains an area of ongoing need.1,4,19
Pairing complementary therapies along with conventional ones in an integrative approach may allow for better and broader targeting of the pathogenic components of AD.
For example, botanicals such as sunflower oil, coconut oil, and oatmeal have been identified as effective in supporting the maintenance and restoration of the skin barrier.20–22 Similarly, wet wrap therapy and balneotherapy (therapeutic bathing) have demonstrated comparable benefits, contributing to improved skin hydration and reduced inflammation.23,24 These approaches are particularly appealing to patients seeking non-pharmacological options that align with their preferences for more natural and holistic care.
In addition to topical therapies, oral supplementation has emerged as another critical component of integrative treatment for AD.25–31 L-histidine, hempseed oil, traditional Chinese medicine (TCM) herbs, essential fatty acids (EFA), and vitamin D have shown potential in modulating immune responses and reducing inflammation, providing additional avenues for therapeutic intervention.25–31 Vitamin E also has anti-inflammatory and antioxidant properties.32 Studies have demonstrated that in patients with AD who were administered 400 IU of vitamin E daily for 4 months, the patients experienced greater improvement in their symptoms compared with those patients taking placebo in terms of reducing itching, severity of atopic dermatitis score (SCORAD), and extent of lesion which was characterized by erythema, edema, excoriation, and lichenification.32
Additionally, probiotics have demonstrated substantial benefits in patients with AD, although the overall body of evidence remains somewhat inconsistent.33,34 They may decrease epithelial permeability to pathogens and their products with the end result of decreased inflammation leading to measurable changes in the SCORAD for patients with AD who take probiotic mixtures.35
Other topical treatments have advantages as well. Black tea compresses have demonstrated a significant decrease in eczema severity and itch.36 Although incompletely understood, black tea is known to contain astringents such as tannins and flavonoids that possess anti-inflammatory properties.36 Vitamin B12 cream has also demonstrated meaningful efficacy in treating AD across multiple ages and appears safe, without any significant side effects.37,38 Similarly, indigo naturalis, formulated as a cream, was found to decrease eczema severity significantly compared to vehicle control.39
In addition to topical and oral therapies, behavioral interventions have shown promise in managing AD.1,4,19 Habit reversal therapy, a behavioral technique that encourages performing another action when having the urge to scratch has shown impressive results in patients with AD.1 Techniques such as nightly massage therapy, relaxation exercises, meditation, and hypnotherapy can help alleviate stress, which is often a significant trigger for AD flares.1,4,19 These therapies promote overall well-being by reducing anxiety and improving sleep, which can directly impact skin health.1,4,19 Acupuncture, an ancient practice rooted in TCM, has also been explored as a complementary approach for AD, with studies suggesting that it may help modulate immune responses and reduce inflammation.1,4,19 Incorporating these behavioral interventions into a comprehensive treatment plan can offer patients a holistic approach to managing AD, enhancing both physical and mental health.
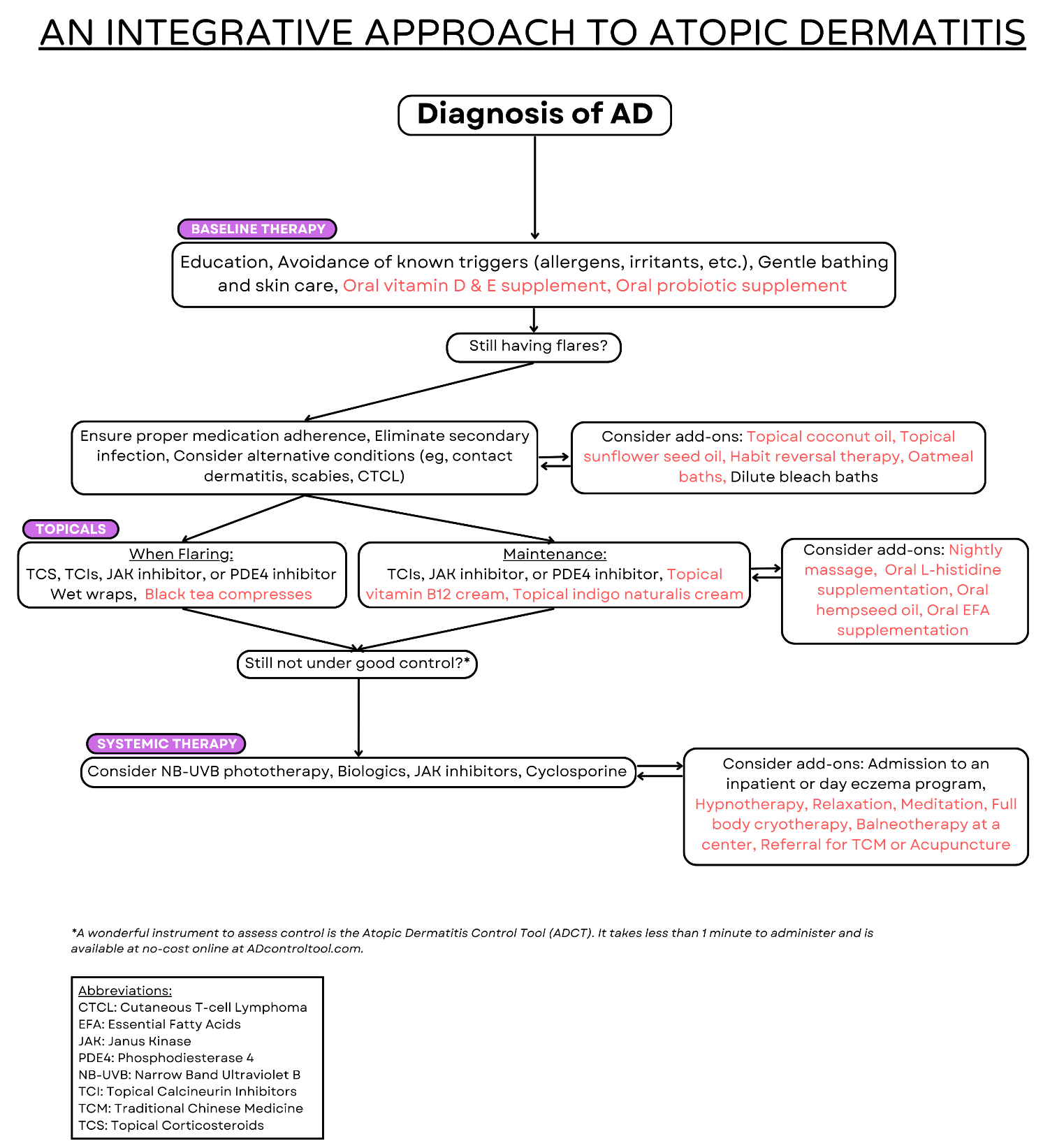
Tailoring therapy to the individual needs of each patient is crucial, as AD presents differently in every person, and the effectiveness of integrative treatments can vary accordingly. An important caveat is that AD affects patients of all ages. While some evidence exists for each intervention described—just as with conventional medications—the majority of studies have been conducted in adults. Clinicians must therefore be particularly cautious when treating children and infants, as some approaches may not be suitable for pediatric patients. To help navigate these complex options, Figure 1 presents an integrative treatment algorithm as a practical tool for clinical decision-making. While by no means exhaustive, it highlights key areas where evidence-based complementary treatments can be integrated. By adopting this comprehensive approach, providers can offer personalized care that addresses the diverse needs of their patients while expanding the range of therapeutic options available.

Funding Sources
No funding sources were secured for this study.
Disclosures and Conflicts of Interest
Kripa Ahuja and Meghana Sunkara have no disclosures or conflicts of interest. Dr. Lio reports research grants/funding from AbbVie, AOBiome; is on the speaker’s bureau for AbbVie, Arcutis, Eli Lilly, Galderma, Hyphens Pharma, Incyte, La Roche-Posay/L’Oréal, MyOR Diagnostics, ParentMD, Pfizer, Pierre-Fabre Dermatologie, Regeneron/Sanofi Genzyme, Verrica; reports consulting/advisory boards for Alphyn, AbbVie, Almirall, Amyris, Arcutis, ASLAN, Boston Skin Science, Bristol-Myers Squibb, Burt’s Bees, Castle Biosciences, Codex Labs, Concerto Biosci, Dermavant, Eli Lilly, Galderma, Janssen, Johnson & Johnson, Kimberly-Clark, LEO Pharma, Lipidor, L’Oréal, Merck, Micreos, MyOR Diagnostics, Regeneron/Sanofi Genzyme, Skinfix, Theraplex, UCB, Unilever, Verrica Yobee Care; stock options with Codex, Concerto Biosciences and Yobee Care. In addition, Dr. Lio has a patent pending for a Theraplex product with royalties paid and is a Board member and Scientific Advisory Committee Member of the National Eczema Association.